Gastrojejunostomy & Vagotomy
. Mr.B. is received from O.R. after G.J.Vagotomy.
a) Discuss the complications following G.J. Vagotomy. (5)
b) Discuss the post operative nursing management of Mr.B. applying the nursing
process. (10)
Definition
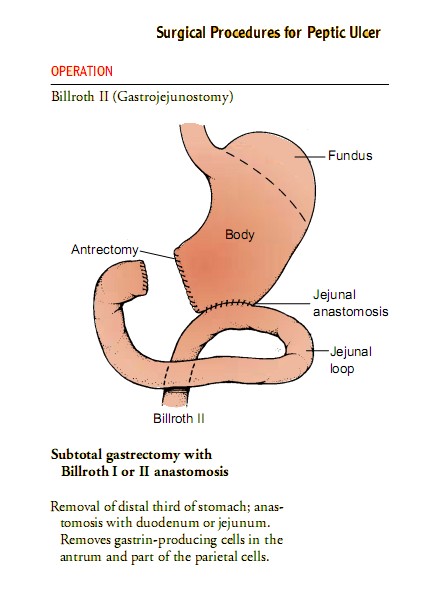
Gastrojejunostomy is an operation to bypass the pyloric sphincter
It is combined with anterior and posterior vagotomy for the purpose of reducing the acid secretions in the stomach : for treating peptic ulcer in the olden days. After the advent of modern drugs like ranitidine and pantaprazole the vagotomy operation has become oblolete.
But gastrojejunostomy is still in vogue for certain conditions
Indications for Gastrojejunostomy
Gastric Outlet Obstruction due to any cause : Pyloric stenosis, duodenal obstruction due to carcinoma etc.
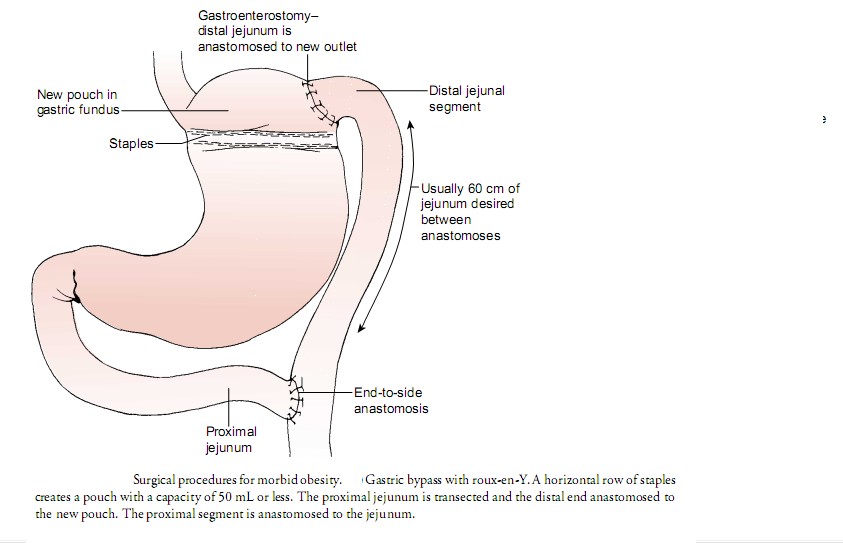
Morbid Obesity : Roux-en-Y gastrojejunostomy (gastric bypass)
Chronic duodenal or prepyloric ulcer with pyloric scarring
Non resectable malignancies of the stomach, duodenum or pancreatic head with GOO as a palliative teatment
Contranidications
Conditions that increase the risk of anastomotic leak (eg. poor nutritional status with seveer hypoalbuminemia or disseminated malignancy with severe ascites or diffus peritoneal deppposits)
Diffuse peritonitis and severe sepsis
extensive gastiric varices
Laparoscopic approach in patients with a past history of operations in the upper abdomen (the presence of adhesions and the altered antomy may complicate the procedure)
Complications following GJ Vagotomy
Jejunal ulccer
Secondary hemorrhage,
Leakage from the anastomosis
Duodenal stump blowout
Infection
Anastomotic stricture
Post gastrectomy syndromes secondary to gastyric resection
dumping syndromes : Early dumping syndrome & Late dumping syndrome
postgastrectomy syndromes secondary to gastric resedction include : Dumping, Metabolic disturbances, Colic, Weight loss, Asthenia
Depending on the time elapsed between the intake of a meal and the appearance of symptoms it is early or late :
Early dumping 30 to 60 minutes postprandially
Prevented by intake of smaller but more frequent meals with reduced sugar content, exercise avoided soon after a meal. Octreotide for medical management
Late dumping : 2 to 3 hours after a meal administer glucose, acarbose,
metabolic disturbances : iron deficiency anemia and vitamin B12 deficiency anemia, impaired fat absorption (steatorrhea and osteoporosis and osteomalacia due to calcium deficiency
Colic in vagoromy
Weight loss is due to negative nitrogen balance. proportional to the amount of sromach resected
Asthenia - in males treated with testosterone
Postgastrectomy syndromes secondary to gastric reconstruction :
Afferent loop syndrome
Efferent loop syndrome,
Retained antrum syndrome,
Alkaline reflux gastritis
Roux-en-Y stasis syndrome
postvagotomy syndromes :
Postvagotomy diarrhea,
Chronic gastric atony,
Icomplete vagal transaction
Postoperative nursing care
Goals :
Relieving pain
Prevent fluid volume deficit
Reduce anxiety
Eliminating infection from the potential or actual disruption of the GI tract,
Maintaining skin integrity
Attaining optimal nutrition.
Post operative nursing interventions :
Intravenous infusion to replace fluid loss and promote adequate renal function
Antibiotic therapy to prevent infection.
Nasogastric suction to prevent paralytic ileus
Place the patient in a semi-Fowlerp osition. This position reduces the tension on the incision and abdominal organs, helping to reduce pain. An opioid : morphine sulfate to relieve pain.
When tolerated, oral fluids.
Any patient who was dehydrated before surgery receives intravenous fluids.
Food is provided as desired and tolerated on the day of surgery.
At discharge teach the patient and family
Arrange the surgeon to remove the sutures between the fifth and seventh days after surgery.
Teach Incision care and activity guidelines
Normal activity can usually be resumed within 2 to 4 weeks.
If there is a possibility of peritonitis, a drain is left in place at the area of the incision. Patients at risk for this complication may be kept in the hospital for several days and are monitored carefully for signs of intestinal obstruction or secondary hemorrhage.