Staphylococcus
1. Describe the clinical findings and diagnosis of staphylococcus aureus in detail.
Definition
Bacteria commonly found in the skin and mucous membrane
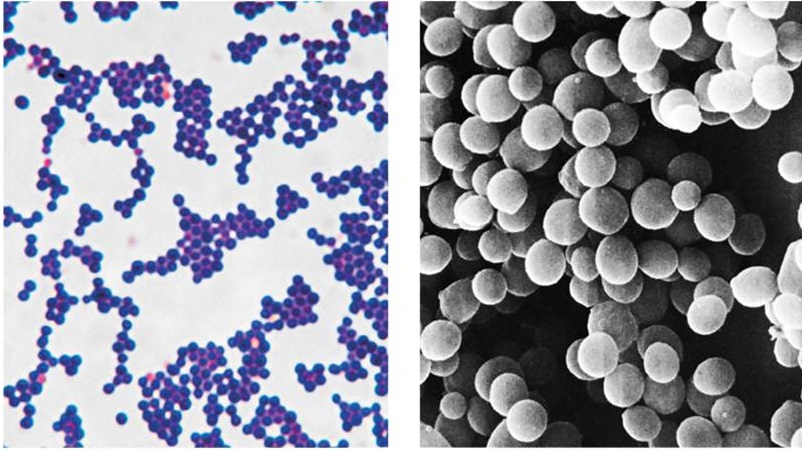
Spherical cells arranged in irregular clusters
Gram positive
No spores no flagella
May have capsules
31 species
Staphylococcus aureus
Grows in large round opaque colonies
Require optimum temperature of 37øC
Facultative anaerobe
Withstands high salt, extremes in pH and high temperatures
Carried in nasopharynx and skin
Produces many virulence factors :-
Enzymes
Coagulase - coagulates plasma and blood; produced by 97% of human isolates : diagnostic
Hyaluronidase - digests connective tissue
Staphylokinase - digests blood clots
DNase - digests DNA
Lipases - digest oils; enhances colonization on skin
Penicillinase - inactivates penicillin
Toxins
Hemolysins (α,β,γ,δ) - lyse red cells
Leukocidin - lyses neutrophils and macrophages
Enterotoxin - induce gastrointenstinal distress
Exfoliative toxin - separates the epidermis from the deris
Toxic shock syndrome toxin (TSST) - induces fever, vomiting, shock, systemic organ damage
Epidemiology and Pathogenesis
Present in most environments frequented by humans
Readily isolated from fomites
Carriage rate for healthy adults is 20-60%
Carriage is mostly in anterior nares, skin, nasopharynx, intestine
Predisposition to infection include : poor hgiene and nutrition, tissue inmury, preexisting primary infection, diabetes, immunodeficiency
Increase in community acquired methicillin resistance - MRSA
Staphylococcal Disease
Range from localized to systemic
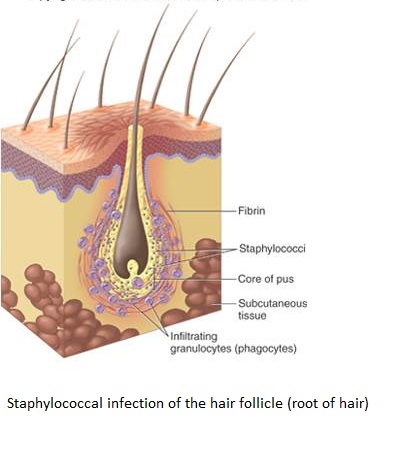
Localized cutaneous infections - invade skin through wounds, follicles, or glands
-folliculitis : superficial inflammation of hair follicle; usually resolved with no complications but can progress
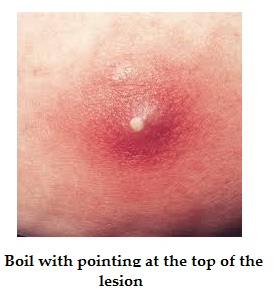
furuncle - boil : inflammation of hair follicle or sebaceous gland progresses into abscess orpustule
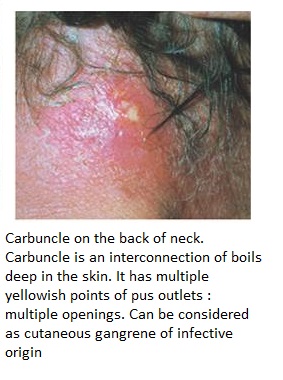
- carbuncle - larger and deeper leson created by aggregationa nd interconnection of a cluster of furuncles
- impetigo - bubble like swellings that can break and peel away; most common in newborns
Systemic infections
- osteomyelitis : infection is established in the metaphysis; abscess forms
- Bacteremia : primary origin is bacteria from another infected site or medical devices; endocarditis possible
Toxigenic disease
-Food intoxication : ingestion of heat stable enterotoxins; gastrointestinal distress
-Staphylococcal scalded skin syndrome : toxin induces bright red flush, blisters, then desquamation of the epidermis
-toxic shock syndrome : toxemia leading to shock and organ failure
Other staphylococci
Coagulase-negative staphylococcus; freuently involved in nosocomial and opportunistic infections
S. epidermidis : lives on skin and mucousmembranes; ednocarditis, bacteremia, UTI
S.hominis : lives aroud apocrine sweat glands
S.capitis : lives on scalp, face, external ear
All 3 may cause wound infections by penetrating through broken skin
S.saprophyticus : infrequently live on skin, intestine, vagina, UTI
Identification of Stapylococcus in samples
Frequently isolated from pus, tissue exudates, sputum, urine and blood
Cultivation (C & S = culture and sensitivity test), catalase, biochemical testing, coagulase
Clinical concerns and treatment
95% have penicillinase and are resistant to penicillin and ampicillin
MRSA - Methicillin resistant S.aureus - carry multiple resistance
Abscesses have to be drained
Systemic infections require intensive lengthy therapy
Prevention
of Staphylococcal infections
universal precautions by healthcare providers to prevent nosocomial infections
Hygiene and cleansing
* * * * * * *