Cord Prolapse
Definition
Umbilical cord prolapse is a life threatening event for the fetus and requires immediate intervention
Cord Prolapse
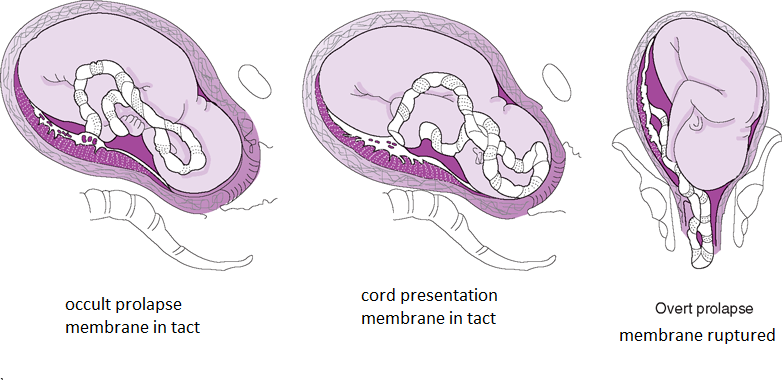
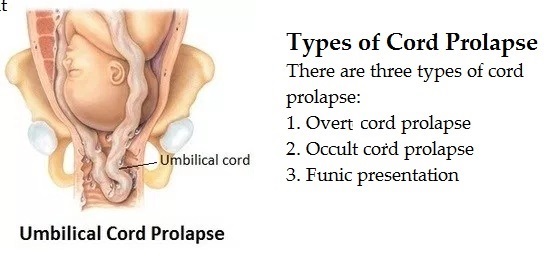
Umbilical cord comes out through the cervix in the presence of ruptured membrane
If the cord is alongside the presenting part - called Occult
If past the presenting part or in front of the presenting part - called Overt
It gets compressed between the presenting part and the pelvis or cervix
Cord presentation
Cord is below the presenting part with intact membrane
Incidence
1 in 265-600 births
Risk factors
for umbilical cord prolapse include
Amniotomy with a high presenting part
Premature rupture of membranes
Long umbilical cord
Fetal malpresentation - breech, transverse lie
Preterm, low birthweight (LBW), or small for gestational age (SGA) fetuses
Multiple pregnancy
Polyhydramnios
Cephalopelvic disproportion (CPD) that prevents fetal engagement
Lack of engagement prior to the onset of labor
Multiparity
Clinical Presentation
May occur prior to or during delivery of the fetus, but it often occurs when the membranes rupture (ROM)
It may be Completely occult prolapse - the cord not visible or palpable and is located between the presenting part and the pelvis or cervix. There may be changes in fetal heart rate tracing
Or Cord presenting in front of the fetal head; may be seen in the vagina and is palpated during a vaginal exam
Or Frank breech presentation with prolapsed cord
The station of the presenting part may be 0 to -4 cm
Pressure on the cord causes oxygen deprivation to the fetus and can result in fetal death
The first sign of umbilical cord prolapse is usually - A severe, prolonged, fetal bradycardia
OR A change from a normal fetal monitor tracing to severe variable decelerations
Predisposing factors
Interventions that may predispose the woman to developing an umbilical cord prolapse include
Artificial rupture of membranes
Internal scalp electrode application
Intrauterine pressure catheter insertion
Manual rotation of the fetal head
Amnioinfusion or amnioreduction
External cephalic version with ruptured membranes
Application of forceps or vacuum
Clinical Management
Prevention
prevention of cord prolapse or its effects
1. Admission if
a. Transverse, oblique or unstable lie after 37 + 6 w
if admission is refused : advised to present quickly if there are signs of labour or suspicion of membrane rupture
(labour or ruptured membranes in the context of an abnormal lie is an indication for Caesarian Section)
b. Noncephalic presentations and preterm prelabour rupture of the membranes
2. Avoid ARM if
presenting is mobile
3. If ARM is necessary it is performed wwith arrangements for immediate CS.
4. Go for CS when cord presentation is seen in established labor
Admission assessment
Fetal presenting part and station
Cervical dilatation
Status of the membranes
Fetal heart rate, pattern, variability
History for presence of the above listed risk factors
Ambulation
Consider discontinuing ambulation if -
Risk factors are present
The membranes are ruptured
The presenting part is engaged
At the time of ROM -
Initiate electronic fetal monitoring if not already in use
Perform a vaginal exam
Management of Prolapse
When the prolapse is identified keep hand in the vagina to push the presenting part away from the cord until the infant is delivered
Continue to palpate for pulsation of the cord
If the cord has prolapsed out of the vagina, keep it moist
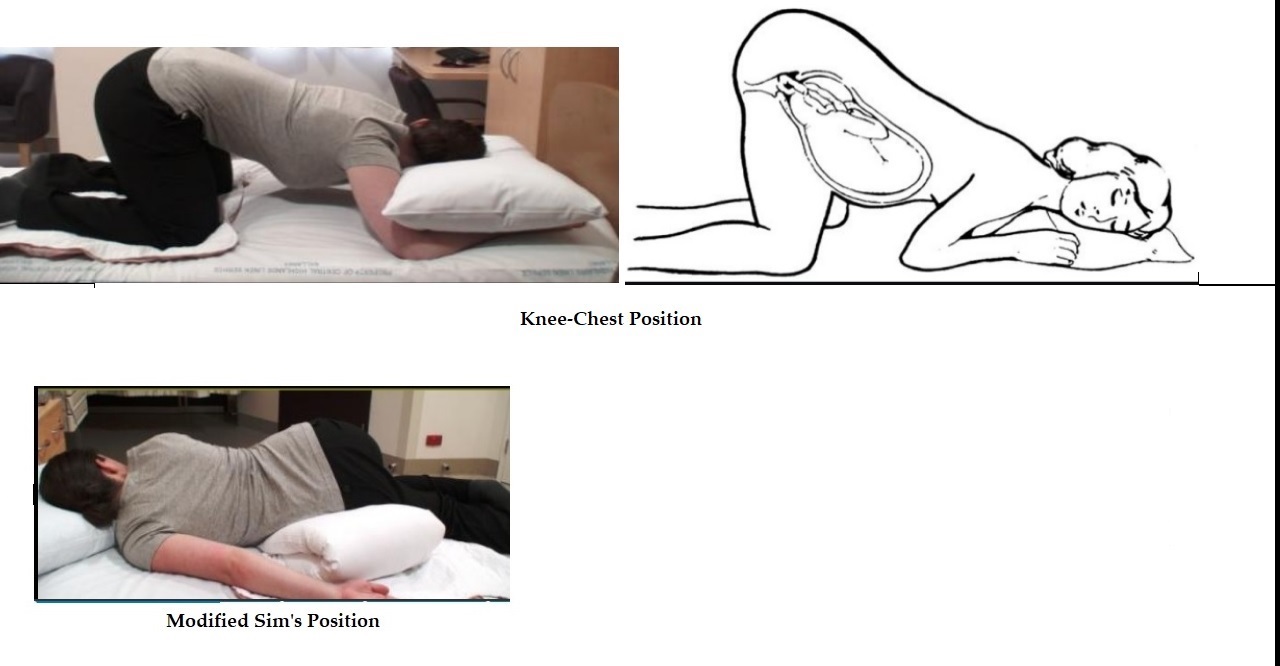
Sterile Vaginal Exam (SVE) to Relieve Pressure on the Umbilical Cord
Manually
Filling the urinary bladder
Knee-chest position
Trendelenburg position
Modified Sims position - patient in side-lying position with hips elevated on pillows
Administer 100% oxygen by face mask
Continuously monitor the fetal heart rate
Prepare for immediate delivery -
Forcep vaginal delivery if the cervix is fully dilated
The fetus is delivered by emergency Cesarean if the cervix is not fully dilated or the fetus in distress,
Potential Complications
Maternal
Trauma to the birth canal from a rapid forceps delivery
Uterine atony with subsequent postpartum bleeding from general anesthesia
Blood loss from Cesarean birth
The usual concerns following any type of surgery (e.g., infection, ileus)
Fetus/Newborn
Fetal anoxia that results in long-term neurologic delays/deficits for the infant
Neonatal infection
Fetal/newborn death
The longer the cord prolapse persists, the greater the risk of mortality for the fetus/newborn
* * * * * * * * * * *